The verdict handed down to the former neonatal nurse Lucy Letby last week brought to an end more than 21 months of court proceedings. After two trials and two attempts to appeal, Letby has been convicted of murdering seven babies and attempting to murder seven others. She is serving whole-life sentences.
For many there has been little room for doubt that Letby is the worst child serial killer in British history. Jurors heard harrowing testimony from the parents of the babies who died, and were shown notes scrawled by Letby and shift rotas that were used to condemn her.
Throughout the trial period, and much of the preceding six years when Cheshire police were investigating a cluster of baby deaths at the Countess of Chester (CoC) hospital and had arrested Letby, laws intended to ensure juries are not influenced by stories in the press meant British journalists reported only what was said in court.
Outside court, however, there has been a growing chorus of voices raising questions about some of the key evidence presented in the trial.
There was no forensic evidence to prove her guilt and no one saw Letby – who continues to maintain her innocence – causing harm.
That also applied to the retrial that reached a guilty verdict last week. Although one of the doctors concluded that she must have tampered with the breathing tube of a baby on three occasions, he did not actually see her doing it.

The prosecution’s case instead drew on accounts from doctors and nurses on the hospital’s neonatal unit and relied heavily on statistical evidence and expert opinion on complex medical points, some of which took days to explain to the lay jury. It is these opinions that some clinicians claim do not stand up to scrutiny.
The case was high-profile and emotionally charged. Successive juries and the families of the babies who died are convinced Letby was responsible. While few of the experts the Guardian spoke to went as far as to say they believed Letby was innocent, the questions about the evidence called into doubt, they said, the safety of the convictions.
A Guardian investigation has interviewed dozens of these experts and seen further evidence from emails and documents. Those raising concerns include several leading consultant neonatologists, some with current or recent leadership roles, and several senior neonatal nurses. Others are public health professionals, GPs, biochemists, a leading government microbiologist, and lawyers. Several of those still working in the NHS have asked to remain anonymous, fearing the impact if they are named.
These experts said they were acutely aware of the suffering of the families involved and did not want to reopen their trauma, but were so troubled they felt compelled to become involved.
Prominent statisticians have described as fallacious a shift table shown to the jury implicating Letby because she was the “one constant presence” when babies died or collapsed.
The Guardian also conducted interviews over several hours with the lead prosecution witness, Dr Dewi Evans, and the specialist instructed for the defence, the neonatologist Dr Mike Hall.
Now, with the second trial over, the Guardian can report these concerns for the first time.
A unit understaffed

In 2013-14, the CoC neonatal unit had four deaths each year. Then, between June 2015 and June 2016, an unusual cluster of 13 deaths occurred. (The hospital has given different accounts of the number and dates of the deaths on different occasions, stating 15 deaths in an earlier response to a freedom of information request.)
The hospital, worried by the deaths, commissioned a review from the Royal College of Paediatrics and Child Health (RCPCH) in July 2016. It found the unit was very short of nursing staff and that consultants were spread too thinly between the paediatric ward and the neonatal unit.
Junior staff did not feel they could call in consultants, often leaving the unit in the care of mid-grade doctors, many of whom lacked sufficient experience, the review reported.
Doctors were surprised by babies collapsing when they did not expect and dying when they could not explain why. Some of the most senior consultants began suspecting that Letby, who was present when these events happened, was responsible.
After further deaths in late June 2016, Letby was removed from neonatal duty. Around the same time, the hospital management downgraded the unit, so that it stopped taking the most premature babies with the highest risk of mortality. The number of deaths fell thereafter.
Fearing that Letby would be allowed to return to the unit, consultants went to Cheshire police in April 2017, and triggered what would become the largest British child murder investigation of modern times.
Concerns over evidence
The initial trial lasted 10 months.
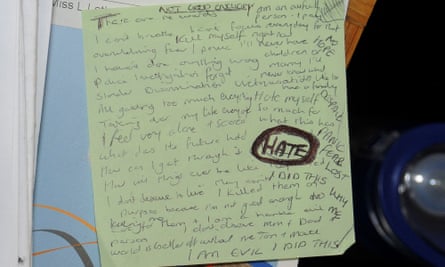
Much was made of notes written by Letby. Despite these saying: “I AM EVIL I DID THIS” and “I killed them on purpose because I am not good enough”, which the prosecution relied upon as amounting to a confession, she has never formally made one.
The notes also included the words: “Kill myself right now … hate my life, fear, panic, despair, WHY ME? I haven’t done anything wrong,” suggesting a state of extreme distress.
There was no apparent motive and no psychological background that matched a serial killer.
Over many weeks through last year’s trial, doctors and nurses involved in the care of the babies explained reams of clinical notes made at the time.
Underpinning this circumstantial evidence were complicated medical opinions presented in court by six expert witnesses. Two others made written statements on specific points.
It is this medical evidence that is at the heart of the concerns voiced to the Guardian, aspects of which have been said to be “implausible” or “medically inaccurate”.

Those who spoke to the Guardian did not do so lightly. Many babies died or collapsed and families have suffered for years.
Several people who voiced their concerns also recognised that they did not sit through the proceedings and did not have access to the extensive case notes used by the expert witnesses – though, during the long trial, detailed accounts of the medical histories of each baby emerged.
They were also aware that several of their questions about evidence had been raised by Letby’s defence in her trial and as core elements of her applications to appeal. Last week, the appeal court – the second highest in the land – published a detailed account of why three judges had strongly rejected all of them. And yet many continued to be sceptical.
Hall is one of those. He provided expert opinion for the defence. He saw the CoC case notes, wrote a detailed report and was at the trial every day bar a couple of half days. His opinion was not heard by the jury as he was not called to give testimony. He does not know why.
He told the Guardian that he was deeply troubled by the case: “With regard to the medical evidence, I don’t think the prosecution proved she was guilty beyond reasonable doubt. I don’t think she had a fair trial because no medical expert witness was called for the defence to challenge the prosecution expert medical evidence.”
The insulin poisoning verdicts
The prosecution alleged there were two principal ways in which Letby inflicted harm: insulin poisoning and injecting air into babies to cause a fatal air embolism.
Letby was found guilty of sabotaging two babies by giving them synthetic insulin, causing them to suffer dangerously low blood sugar levels (hypoglycaemia).
The insulin cases were the first on which the jury reached a verdict, of attempted murder, and they were unanimous. Both babies survived.
Judge Goss directed the jury that if they concluded that Letby had deliberately harmed babies one way, they could also conclude that she had inflicted deliberate harm on others, even if jurors were not certain of her methods.
The prosecution presented two test results, the only empirical scientific evidence in the case. An expert witness in court – who, when approached by the Guardian, said he could not comment – said the test results indicated that a steady flow of synthetic insulin had been administered. Biochemists testified in court that the lab that conducted them was accurate and working well.
But while the test results had provided a helpful clinical guide for diagnosing hypoglycaemia, the type of test used does not measure insulin itself. Instead it measures antibodies to insulin and can cross-react with other molecules.
Several experts challenged the use of results from this type of immunoassay test as evidence of crime, including the forensic scientist Prof Alan Wayne Jones, who is one of Europe’s foremost experts on toxicology and insulin. He has written about the limitations of immunoassay tests in criminal convictions, and said they needed to be verified by a more specific analytical method to provide binding evidence in criminal cases.
The defence never asked the biochemists whether the test was the right kind to prove insulin poisoning.
This and what people felt were fundamental errors in interpreting the insulin results were raised in detailed papers submitted to the court of appeal by a group of experts, including a consultant neonatologist, a medico-legal expert, a chemical process engineer and a former public health director. Their intervention was rejected as inadmissible and not considered by the court.
Air embolism
The lead expert witness called by the prosecution was Evans. He left clinical practice in 2009, but has more than three decades’ experience working in the courts and became a consultant paediatrician in his early career. He helped establish a specialist neonatal unit in Swansea in the 1980s.
Letby’s counsel, Ben Myers, applied to have Evans’s evidence dismissed. Among his arguments were that Evans had failed to be impartial and that he had constructed theories designed to support the charges. The trial judge and the court of appeal judges strongly rejected the criticisms, ruling that Evans did not lack impartiality and was well-qualified to give an opinion. They agreed it was for the jury to assess the quality of his evidence.
Evans strongly rejected any suggestion he was biased. “One’s role as a witness is to consider all possible scenarios,” he said, and then to advise the court based on “one’s own experience and other supporting evidence”.
Evans’s analysis concluded that seven babies had been harmed by injecting air into them, causing or contributing to their collapse and death. In some cases, he said injecting air to cause dangerous air embolism was the sole mechanism of murder; in others, he gave additional causes of harm such as deliberate trauma to the liver, or deliberate overfeeding.
There were two parts to his reasoning on air embolism. His opinion was that babies had either had air injected into their stomachs via the tiny feeding tube that newborns often have inserted through the nose, or into their bloodstream through various lines and catheters.
Other prosecution expert witnesses largely agreed with Evans’s opinion on this. But the idea that injecting air into the stomach via a nasogastric tube could cause collapse leading to death was described as nonsensical or “rubbish”, “ridiculous”, “implausible” and “fantastical”, by eight separate expert clinicians who spoke to the Guardian, seven of them specialising in neonatology.

Several said it was not practically feasible. Nasogastric tubes are tiny; it would take several refills using the 10ml syringes on neonatal units to inject a significant quantity of air. Furthermore, it would leak out or the baby would burp or vomit it up, or pass it as wind, they said.
Evans said: “It was a phenomenon I had never encountered previously.” He added that without the full clinical records, others could not comment objectively.
The other half of Evans’s opinion on air embolism was that air was injected into babies’ veins to cause harm. This opinion was accepted as a cause or contributory factor by the jury in five murder verdicts. In some cases, the prosecution said babies had been harmed by both methods.
Evans’s view drew on skin discolorations observed in several of the babies. He referenced a 1989 academic paper by Drs Lee and Tanswell on air embolism in the bloodstream in babies. That paper described skin discoloration that indicated air embolism in babies caused by high-pressure ventilation – quite different circumstances to allegedly injecting air at normal pressure. A second expert witness, Dr Sandie Bohin, reached similar conclusions.
The surviving author of that paper, Dr Shoo Lee, who retired recently from a career as one of Canada’s top neonatologists, was not called by the defence for the first trial but he did give expert testimony in Letby’s appeal in April. Lee said that in his view none of the descriptions of the babies’ skin discolorations used by the prosecution witnesses matched the kind that characterised air embolism.
Lee’s testimony was not admissible by the court of appeal, with the judges saying the defence could have called him in the trial. The judges added that the prosecution’s expert witnesses did not solely rely on skin discoloration to indicate the condition.
Questions over use of statistics
Sir David Davis MP used parliamentary privilege to tell the House of Commons in May about a 13,000-word article in the New Yorker magazine about “the Lucy Letby trial, which raised enormous concerns about both the logic and the competence of the statistical evidence”. The US publication reported what British media were also hearing from experts but could not cover while the retrial was pending.
A key plank of the prosecution was that it was always Letby who was there when the babies collapsed or died unexpectedly.
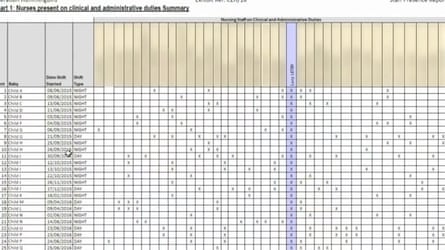
The jury was shown a chart listing 25 deaths and collapses Letby was charged with and the names of the nurses who had worked on the unit through the period of the cluster of deaths. The column for Letby was marked with a cross for every incident, whereas other nurses had only been on shift for a few of them.
However, the jury was not told about six other deaths in the period with which Letby was not charged. They were omitted from the table.
The medical director of the unit, Dr Stephen Brearey, had originally pointed out the statistical coincidence to hospital management, whose response had been that it was just that: a coincidence.
One of the most senior consultant paediatricians at the hospital, Dr John Gibbs, had similar doubts when colleagues at the same time were pointing the blame at Letby, a leaked email shows. He wrote to his fellow clinicians in early July 2016: “The increase in neonatal mortality that we have experienced over the last 18 months might be within ‘expected’ statistical variance (but I’m not sure because my stats isn’t good enough). You might feel that this must be wrong, but it’s all to do with the statistics of small numbers.”

Gibbs, who was a witness of fact in both trials, has accepted foul play. When approached by the Guardian, he said he could not discuss the case in detail, but added that the concern was not only based on the shift chart but also “on the unexpected and unusual nature of many of the deaths”.
In September 2022, the Royal Statistical Society warned that murder accusations in healthcare settings had repeatedly been based on fallacious use of statistics. Its chief executive at the time, Stian Westlake, said some RSS members saw the Letby case as one that could repeat the mistakes of the past.
John O’Quigley, a professor of statistical science at University College London, said: “People get the wrong end of the stick with statistics. In my opinion there was nothing out of the ordinary statistically in the spike in deaths, and all the shift chart shows is that when Letby was on duty, Letby was on duty.”
Richard Gill, an emeritus professor of mathematics at Leiden University in the Netherlands, was involved in two cases similar to Letby’s in which statistical coincidence was wrongly used in part to convict two nurses of murdering their patients: Lucia de Berk, a neonatal nurse in the Netherlands, and Daniela Poggiali in Italy. Their convictions were eventually quashed, thanks in part to Gill’s contributions.
Gill, who has drawn much criticism for pointedly posting on social media during the trial that the Letby shift table was meaningless and that she had suffered a miscarriage of justice, said: “The police investigation and crown prosecution made all the mistakes the RSS warned about. Nobody studied the statistics in a professional way.”
The police said it was not appropriate to comment when further investigations were continuing. The CPS said two juries and four appeal court judges had reviewed the evidence against Letby. “The court of appeal rejected her argument that expert prosecution evidence was flawed,” a spokesperson said.
Could there be other explanations for the deaths?
In autumn 2016, after the royal college report, Dr Jane Hawdon, the lead consultant neonatologist at the Royal Free hospital in London, looked at the cluster of deaths and collapses. Her review did not look at all the clinical notes, but leaked documents seen by the Guardian suggest that in 13 of the cases Hawdon reviewed she found the babies had received suboptimal care and the “death/collapse is explained but may have been prevented with different care”.
In four of the cases, the “death/collapse was unexplained” and she advised a deeper forensic review. The Guardian understands that another consultant neonatologist did then review the cases that were unexplained. Evans said her findings differed from his. She declined to comment.
CoC said it was unable to comment while other investigations and an inquiry were continuing.
Hall, the expert for the defence, said that in his view the prosecution witnesses “exaggerated how well arguably all the babies who sadly died were”, a point denied by Evans. Hall questioned the plausibility of air embolism, and said six of the seven babies found to have been murdered had postmortems at Alder Hey hospital, a centre of excellence. These pathologists had had the advantage of physically examining the babies and reported no unnatural findings.
Evans said the defence could have called expert witnesses to challenge his and others’ opinion in court but they did not.
The defence team declined to comment.
Many of those who spoke to the Guardian felt strongly about their concerns, but few knew where to take them. It is understood that several complaints focusing on the evidence given in the trial have been put into the medical regulator, the General Medical Council, by some who wanted to have their concerns recorded.
Dr Svilena Dimitrova, an NHS consultant neonatologist who is part of the government-appointed Ockenden review investigating deaths and harm allegedly caused to dozens of babies in Nottingham University NHS hospital trust, is one of five who the Guardian understands has approached the GMC in relation to evidence given by Evans. She said she took this step having been approached by multiple consultant neonatologists and paediatricians, and specialist neonatal nurses, who flagged up their concerns to her but were frightened to go public.
She said that in her opinion, “the theories proposed in court were not plausible and the prosecution was full of medical inaccuracies. I wasn’t there, so I can’t say Letby was innocent, but I can see no proof of guilt”.
“There are fundamental flaws in the justice system when it comes to prosecuting healthcare professionals, which mean that it does not address systemic NHS failures and blames individuals instead … The information presented to court was flawed and not proof of guilt beyond doubt,” she added.
Roger Norwich, a medico-legal expert with an interest in paediatrics and newborns, has also made complaints to the GMC. He has put in a complaint about Evans, and has also put in a complaint about the second witness, Bohin. He said he thought both had failed to provide balanced, impartial views, instead giving the court “opinions that would not be supported by most doctors”. Both Dimitrova and Norwich said they had not yet received a response to their complaints from the GMC.
Anyone can make a complaint to the GMC if they have concerns about a doctor, but most are not investigated by the regulator.
Neither Dimitrova nor Norwich had access to the full clinical notes.
Bohin responded to the issues raised: “Everyone is entitled to their opinion, yet not everyone had access to all of the information in this case. I did and this informed my reports and subsequent opinions.”
Evans said he had never been told of any medical inaccuracies and was not aware of the GMC complaints until he was contacted by the Guardian. He described them as vexatious in an article in the Sunday Times. He told the Guardian: “My opinion was based on evidence. If they have not seen the original documents, their opinion is based on opinion.”
He added: “It is understandable that a trial of this sensitivity will create conflicts of views. Wanting to shoot the messenger is not an unsurprising response, especially given the criminal justice system’s record of miscarriages of justice.”
Like Gill, Prof John Ashton, a former public health director, became exercised about Letby’s trial before it was finished. He had blown the whistle on a cluster of baby and maternal deaths at the Morecambe Bay hospitals when he was regional director of public health for the north-west of England. His direct experience, with the Morecambe Bay scandal, is that human instinct drives people to look for someone or something to blame, but the root causes are often more complicated and numerous.

“You don’t need a serial killer to account for what happened at Chester. Disasters, and this was a disaster, generally happen as a result of the convergence of a number of factors … We’re talking in Chester about system failure – it was a hospital that was not well run, that had ambitions beyond its capability, that had problems with clinical governance and environmental problems.”
He added: “The arguments about Lucy Letby herself boil down to the fact that circumstantial evidence, and statistical and expert witness evidence that I believe was seriously flawed, were presented to the court.”
Source: theguardian.com


