Thirteen days before her alleged rapist was due to stand trial, Jade McCrossen-Nethercott received devastating news. After three years of waiting, the Crown Prosecution Service was abandoning the case.
It was not for lack of evidence. After the alleged attack, McCrossen-Nethercott had gone straight to the police, who took her clothes, phone, and swabbed her “head to toe”. Then there was her broken necklace, the marks on her arms, the no-comment interview the suspect gave after he was arrested and the allegation that a drink he gave her had tasted strange.
Instead, a sleep expert appointed by the defendant’s legal team had produced a last-minute report opining that rather than being raped while she slept – as she alleged – there was a possibility she was suffering from a bout of “sexsomnia”. The rare sleep disorder could have caused her to have sex while asleep, leading the man accused of raping her to believe she was consenting.
McCrossen-Nethercott was baffled. She had never heard of sexsomnia, let alone been diagnosed with it. Like one in five people, she had sleep-walked as a child, and sometimes sleep-talked after nodding off as an adult. But none of her romantic partners had noticed anything odd about her sexual behaviour, and there was nothing in her medical history to suggest she had a problem.
The 32-year-old, a client care manager for the British Pregnancy Advisory Service, was troubled by how conclusive the diagnosis sounded. The defence-appointed expert Dr Zenobia Zaiwalla had said there was a “strong possibility” she had suffered an episode of sexsomnia.
But Zaiwalla had never met or clinically assessed her, nor read her medical history. She hadn’t spoken to McCrossen-Nethercott’s partner, family or friends – or ordered sleep tests. Her opinion appeared largely based on the defendant’s statement, comments McCrossen-Nethercott had made in a police interview, and a written questionnaire she had later been asked to complete, including whether she snored (yes), woke up gasping and choking (no) or had experienced sleep walking as an adult (no). “It felt like it was plucked out of thin air,” McCrossen-Nethercott said.
Another sleep expert, appointed by the prosecution, wrote that, while he had “no material differences of opinion” to Zaiwalla, and agreed sexsomnia was possible, he believed McCrossen-Nethercott may have been drugged with a substance like GHB, which would not show in urine samples taken the morning after the incident due to its short half-life. It would explain why she had no memory of what happened, and how her clothes had been removed, and the accused able to penetrate her, without her waking up.
But a seed of doubt had been sown. In a letter to McCrossen-Nethercott in October 2020, a senior crown prosecutor wrote that there was “no longer a realistic prospect of conviction”. When the trial date arrived, the prosecution offered no evidence. The defendant was acquitted and the case thrown out.
In the months that followed the collapse of the trial, McCrossen-Nethercott became suicidal. She suffered flashbacks and panic attacks and turned to drink and prescription drugs to cope. “It took me to the darkest points, more so than I’d ever experienced. My kind of sense of self was completely obliterated,” she said.
As she battled to get better, she immersed herself in the world of sexsomnia. She spent hours researching the condition, learning how it typically occurs during non-REM sleep – the deepest stage of the sleep cycle – and is potentially caused by a disruption in the brain.
She learned how it is a relatively new diagnosis, with 94 cases documented worldwide by the time of a 2015 study (although experts believe the true figure could be far higher). She also learned that research into the disorder was extremely limited: scientists were unclear on its exact cause, prevalence, and triggers.
The facts they did agree on seemed to have few parallels to her own case.
On the night of the alleged attack in March 2017, McCrossen-Nethercott had been to a south London bar for a friend’s birthday, before several of the group went back for drinks at the defendant’s home. Everyone had been drinking, but witnesses said McCrossen-Nethercott only appeared tipsy; there was nothing to suggest she was severely intoxicated. McCrossen-Nethercott told police that as it got late, the defendant offered her his bed. She declined, fearing it would send the wrong signal, and nestled on the sofa beneath a blanket instead.
About three hours later she woke up, partially undressed, and with no memory of what had happened but an “immense feeling of being violated”: “not necessarily knowing what had penetrated me, but knowing that something had”. She said: “My pants were off, my bra was unpinged at the back, and my necklace was broken.”
She said she angrily confronted the only other person in the room, who appeared dazed and left quickly. McCrossen-Nethercott gathered her things and ran to the nearest bus stop, calling her best friend on the way. “I said to her, ‘I think I’ve been raped.’”
When the accused was first interviewed by police, he initially answered “no comment”. After the swabs found his semen inside her, he was interviewed again and gave a statement that sex had happened but it was consensual, before returning to answering “no comment”.
In her interviews, McCrossen-Nethercott gave a detailed account. She explained how it had not been a problem for her to get to sleep on the defendant’s sofa because she was “quite a good sleeper”. “When I’m on a plane I am asleep before we take off,” she told the police interviewer.
Asked to expand, she explained that she often snored, and that once, while on holiday years ago, she had not heard a fire alarm going off in the night. She also said that she had sleep-walked when she was a child, and sometimes sleep-talked.
The comments would later be seized upon by the defence, and used as evidence she did have sexsomnia. But McCrossen-Nethercott’s own research was now casting doubt on that diagnosis.
She found that sleep-walking as a child and sleep-talking were indeed potential precipitating factors for sexsomnia – as was loud snoring, which the experts said could indicate sleep apnoea. But all those conditions were fairly common. The link was far from conclusive.
She also read studies suggesting that while it was rare for men to be diagnosed with sexsomnia, it was even rarer for women. And when they did have it, they were more likely to engage in masturbation rather than full sex.
Other research indicated sexsomnia episodes often occurred when the person was in familiar surroundings, such as their own home or bed.
McCrossen-Nethercott also read about the phenomenon of sleep rape. In her interviews with police, she had expressed disbelief that the accused had managed to remove her underwear and penetrate her without waking her up. It was something Zaiwalla drew upon in her report: if she didn’t have sexsomnia, then when she was being attacked, why didn’t she stir?
The CPS expert also took this as evidence to “support the account that she cooperated with the sexual activity, indicating either consent, parasomnia or drug-facilitated pseudo-consent”.
McCrossen-Nethercott discovered research indicating that it was not uncommon for those experiencing “sleep rape” to remain asleep throughout. In one analysis of police reports about 39 sleep rape cases, four of the victims “were entirely unaware that they had been … penetrated by the suspect”. “To some, it might seem impossible that such rapes could occur without waking the victim, but the filming of such attacks by offenders means such denials lack credibility,” the 2022 study, by academics at De Montfort and the University of the West of England, concluded.
She also discovered that sexsomnia had popped up in criminal cases – but typically used by the defendants. Hers is the only known case in the UK where the alleged victim was said to have the condition, but dozens of defendants had used it as part of their explanation for alleged crimes – including rape, assault, child sexual abuse and domestic violence.
It often presented a quandary for juries. By law, if they found that an accused person was in such a state – known as “automatism” – when they committed an alleged offence, they had to be found not guilty because their behaviour was involuntary.
But many of those successfully pleading sexsomnia in court had no known history of the condition and no prior diagnosis. Sometimes, cases involved defendants performing a complicated series of actions in unfamiliar settings, which experts said was not typical of genuine sexsomnia.
Sometimes mere mention of the disorder seemed to be enough to sow sufficient doubt to secure a “not guilty” verdict. In one rape case, two expert witnesses said evidence for the defendant having sexsomnia was “weak” but that they could not categorically rule it out. The jury subsequently acquitted the man.
McCrossen-Nethercott’s research left her with questions. If there was evidence of the condition being misused in other cases, why had the CPS not challenged the defence claim of sexsomnia at trial? Why hadn’t the sleep experts assessed her before reaching their views? And what was to stop others using it to discredit victims, or to get themselves off the hook?
“It seemed like it was essentially an easy get-out-of-jail free card,” McCrossen-Nethercott said.
In an interview for a BBC3 documentary about her story, Sexsomnia: Case closed?, McCrossen-Nethercott spoke to barrister Allison Summers KC, who has acted for defendants who used the sexsomnia defence.
She said there was a danger of genuine sexsomnia sufferers being convicted of serious offences that they were not guilty of. There was also a risk that “some guilty people get off”, she said. “The only thing I can say is that you hope the criminal trial process will enable those genuine cases to be pulled out from those less genuine.”
There were other things playing on McCrossen-Nethercott’s mind – like that she had supposedly consented not only to sex while asleep, but to sex without a condom – something that, as a reproductive health specialist, she says she simply wouldn’t do. The fact the accused had been intoxicated on the night – and so his memory may have been impaired – also seemed to have been skirted over. “There were these other details that just didn’t seem to have been discussed,” she said.
Playing on her mind was an even more disturbing concern: what if she really did have sexsomnia?
“As much as I knew deep down that I didn’t, the CPS had kind of planted the seed and it was enough for them to essentially close their case and the [defendant] to walk free,” she said. “So I had this weird back and forth like, ‘Oh my god, do I have this?’ I used to have faith in the system, so I worried it might have some substance.”
Where before she had been a deep sleeper, she developed anxiety around bedtime. She stopped sleeping near family members or friends, in case she had an episode, and although she never had previously, she worried she might initiate sexual activity with her long-term partner without his consent. “I felt like I had to come with a disclaimer,” she said.
after newsletter promotion
She turned to doctors for answers. She spoke to her GP and was referred to a specialist NHS sleep team at Guy’s Hospital in central London, but was turned away because they didn’t deem her to have any sleep concerns. She then tried private specialists, paying for two consultations from separate experts, and undergoing a home sleep study. Soon afterwards, following another referral by her GP, she was accepted for a sleep study at UCL Hospital.
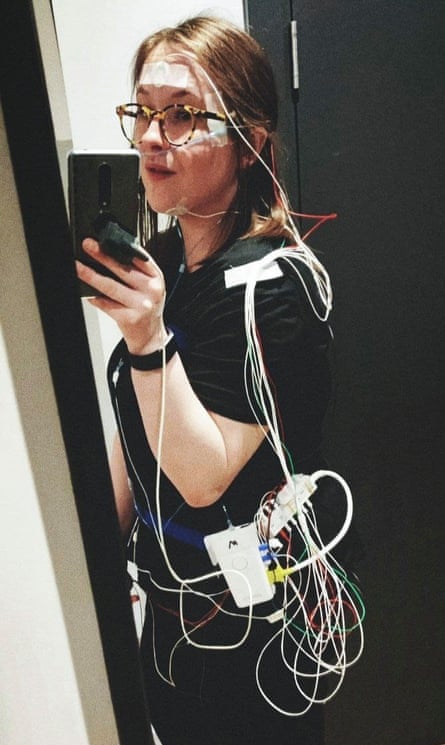
The tests involved her being hooked up to an ECG monitor with wires glued to her head, chest and legs, to monitor her brain activity and movements as she slept. One test was conducted while she was sober, and the other after she had consumed alcohol. The results suggested she may have mild sleep apnoea – a potential trigger for sexsomnia – but found nothing else unusual. “Overnight polysomnography showed good sleep efficiency. There were no features of NREM parasomnia after arousals from deep sleep. In summary, the study did not show any precipitating factors for NREM parasomnia,” a 2022 discharge letter from UCLH said.
Such tests, known as polysomnographies, are not conclusive. Sleep experts say the chance of an abnormal sleep event actually happening during a test is slim, and that it’s impossible to retrospectively prove someone was suffering from an episode of sexsomnia at any given time.
But some experts say it is imperative they are conducted whenever there is a claim of sexsomnia in a criminal case. Prof Colin Shapiro, a global expert on sexsomnia, who first coined the term about 20 years ago, said: “It needs to be done because it really tips the information in a significant way.” He told the Observer earlier this year that he would refuse to appear as an expert witness in a case unless they had been done. “I would say I’m not going to court because I don’t have all the information,” he said.
McCrossen-Nethercott also submitted subject access requests to obtain copies of the reports the sleep experts had written. In them they considered multiple theories, including that she was so drunk she couldn’t remember the incident, which they agreed was unlikely, and that the defendant raped her as she slept, which neither could rule out.
With regard to sexsomnia, Zaiwalla’s report indicated she had based her opinions largely on comments made in McCrossen-Nethercott’s original police interview as well as a 16-question questionnaire she had asked her to complete a few months before the trial.
Other conclusions appeared to draw on the defendant’s statement. In one section, Zaiwalla’s report said McCrossen-Nethercott would have “appeared to be awake, with eyes open and showing pleasure”. In a complaint to the CPS, McCrossen-Nethercott said it was “incredibly troubling” that the comments appeared informed by the defendant’s account, “which cannot be verified”.
The report also indicated that Zaiwalla had been asked by the defence to “opine in the abstract” about whether McCrossen-Nethercott could have been experiencing sexsomnia, rather than to come to a formal clinical view – because an assumption had been made that she was “unlikely to consent to extensive and invasive tests in some sort of sleep clinic”. McCrossen-Nethercott says that, had she been asked, she would have said yes to the tests.“They had my phone, my counselling notes. I didn’t want anything to hinder this getting to court,” she said. “I had been very forthcoming throughout the entire process.”
Zaiwalla, an honorary consultant in clinical neurophysiology, with expertise in paediatric epilepsy and sleep disorders, was contacted by the Observer but said she was unable to comment. “I am sorry I am unable to respond to your queries as I have a duty of confidentiality,” she said.
A second expert report was also released to McCrossen-Nethercott through the subject access request, produced by Dr Neil Munro, a consultant neurologist and accredited somnologist who had been appointed by the prosecution.
Like Zaiwalla, he did not speak to McCrossen-Nethercott directly. His report disagreed with some aspects of the other expert’s conclusions, including comments that there was a “strong possibility” McCrossen-Nethercott had sex with the defendant in a “dissociative state while subconsciously believing she was with her partner”. He wrote: “I do not agree that it is relevant to speculate on whether [she] had subconscious cognitions that equated to a belief she was sleeping with her boyfriend.”
Munro said he could not rule sexsomnia out, adding that snoring and childhood sleepwalking could indicate a predisposition to the disorder, and that the late bedtime, alcohol ingestion and sleeping arrangements were potential “risk factors”. He believed it was possible that such an episode could have been triggered by non-consensual touching by the defendant while McCrossen-Nethercott slept, such as a kiss or other contact.
But Munro also put forward another possibility: that McCrossen-Nethercott had been drugged. Others appeared to have dismissed this theory because samples McCrossen-Nethercott provided after the incident did not show traces of any common date-rape drugs.
But the prosecution expert pointed out that, if she had been spiked with GHB – a central nervous system depressant that causes drowsiness and reduces heart rate – this would be unlikely to show in tests due to its short half-life. McCrossen-Nethercott had been to the toilet several times before her urine sample was taken – so negative toxicology did not rule it out. “A small dose of GHB in conjunction with alcohol would be a potent cause of amnesia,” he added.
He also cited evidence that McCrossen-Nethercott had found a glass of red wine she was given by the defendant “unpalatable”. “GHB tastes salty,” he wrote. “Drug-facilitated sexual assault is a possible explanation of events.” It was not enough. The CPS felt the fact that a second expert could not rule out sexsomnia was enough to fatally undermine the case.
Prosecutors considered approaching other experts to ask their views, but decided not to for fear of being accused of “expert shopping”. Ten days after receiving Munro’s report, they closed the case.
In a statement to the Observer, Munro said the case was “complex”. He raised concerns about due diligence and said greater focus should have been on evidence of potential violence and the possibility of drug-facilitated sexual assault.
He also said his view was that McCrossen-Nethercott’s case should have gone to trial, so the defendant’s position could be challenged, and that she was right to sue the CPS. But he believes it could have been “difficult to obtain a conviction beyond reasonable doubt”, and raised the possibility of unsafe convictions.“There are parasomniacs who are wrongly convicted,” he said.
In response to concerns about the weight given to expert reports in sexsomnia cases, he said acting as an expert witness was a “social duty” and that it was ultimately for the prosecution and defence to test their evidence in court.
“In the end we only help out with the science and what might have happened,” he said. He added that he asked the CPS if he could assess McCrossen-Nethercott directly, but the request was refused.
The CPS said it was committed to improving “every aspect of how life-changing crimes like rape are dealt with”, including “working closely with police from an early stage to ensure we focus on the behaviour and actions of the suspect, not the victim”.
McCrossen-Nethercott will never know whether a jury would have decided to convict. But she has now received confirmation that the CPS decision was wrong.
Last week – three years on from the decision to drop her case – McCrossen-Nethercott received a historic payout and an “unreserved apology” from the CPS, which admitted the sexsomnia claim should have been robustly challenged in court.
Following a review of the case, Malcolm McHaffie, chief crown prosecutor for the Thames and Chiltern area, wrote that “the original decision was made on the basis that the expert evidence could not be overcome. However, the timing and content of the defendant’s account were open to challenge. Therefore the basis on which the experts made their findings could have been undermined and the expert evidence challenged”.
McCrossen-Nethercott said the £35,000 settlement – which covers medical and legal costs, and loss of earnings – was symbolic, and she hoped it would set a precedent. Kate Ellis, joint litigation lead at the Centre for Women’s Justice, said claims from victims against the CPS were “difficult legally”, with payouts “extremely rare”. “It’s a testament to how severe the failing was on the part of the CPS that we have been able to bring this claim,” she told the BBC. But despite the admission of errors, McCrossen-Nethercott has no further route to court. Double jeopardy rules mean that, now the accused has been formally acquitted, he cannot be retried.
She said the settlement had also done little to quell her fear that suspects could use “sexsomnia” to discredit victims – or explain away alleged crimes. Earlier this year, an Observer investigation found evidence that its use is increasing – with 51 known UK cases in the last decade, and eight in the past year alone. In about 60% of cases where sexsomnia was part of the defence, a not-guilty verdict was returned. In at least one case, a man who avoided a rape prosecution after claiming to have sexsomnia went on to attack again.
The investigation also found evidence of the CPS dropping other cases before they reached court. One law firm advertised how it “kept pressure” on the CPS during the prosecution of a wealthy client who had been charged with sexual assault. The charges were dropped before the case went to trial.
At the time, Dr Neil Stanley, an independent sleep expert, told the Observer there was a “strong likelihood of miscarriages of justice”. He said: “I know in my heart of hearts that there are cases where guilty men have got away with it. And that cannot be a legitimate consequence of the system. The system has to change.”
McCrossen-Nethercott no longer has faith in the systems set up to protect victims, and she is haunted by the fact that in her case, a rapist may have walked free.“It’s an immense feeling of being let down,” she said. But if something good is to come from her ordeal, she hopes it is that sexsomnia claims will be more robustly challenged in future – with lab tests, bed-partner interviews, and medical history obtained as a minimum – and that there will be a “frank, public conversation” to ensure potential miscarriages of justice are prevented.
“I would never in my wildest dreams have imagined sexsomnia would be the reason they dropped my case,” she said. “What’s to stop it being manipulated in future?”
Source: theguardian.com


